About Thyroid Nodule
What is thyroid?
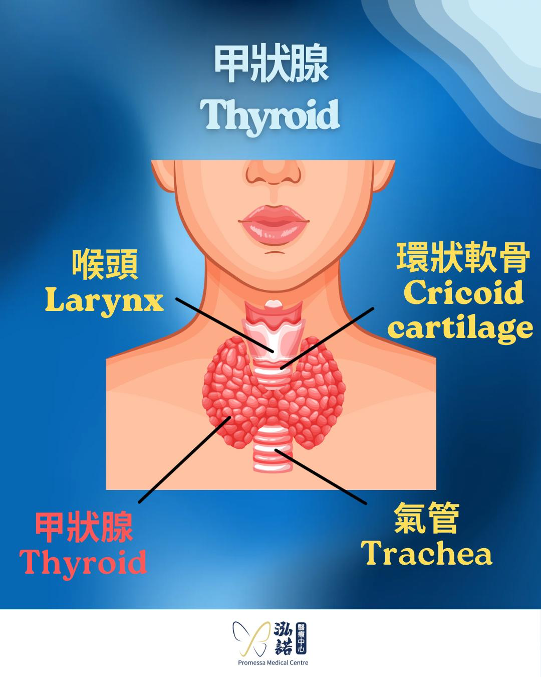
Thyroid is an important endocrine gland in human body. It is a butterfly shaped organ located between the cricoid cartilage and the clavicles in the anterior neck.
It is divided into left and right lateral lobes, situated on both sides of the trachea and connected by the isthmus in the middle which covers the trachea.
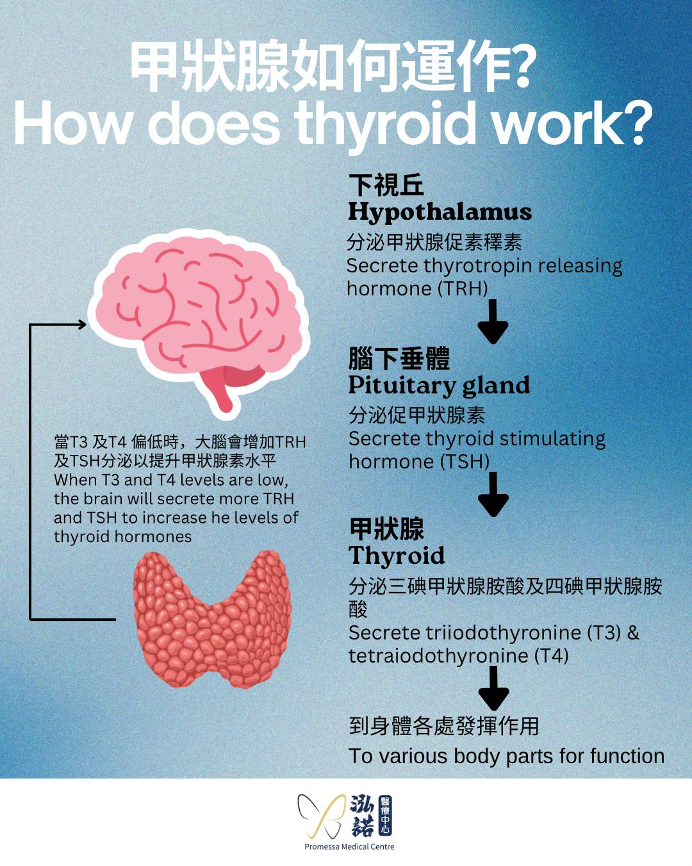
The main function of the thyroid gland is responsible for the production of thyroid hormone (or thyroxine) to regulate various body functions, including:
- Metabolism
- Weight control
- Body temperature regulation
- Blood pressure and heartbeat regulation
How to classify thyroid diseases?
- Functional thyroid disorders
When thyroid gland produces too much or too little thyroxine. For example- too much thyroxine production: hyperthyroidism or thyrotoxicosis
- too little thyroxine production: hypothyroidism
- Structural thyroid disease
Abnormal thyroid tissue growth forming a nodule. For example- benign thyroid nodules
- malignant thyroid nodules (thyroid cancer)
Functional and structural thyroid problems may occur separately or at the same time.
What is a thyroid nodule?
Thyroid nodule is a general term for thyroid lump resulting from abnormal growth of thyroid tissue. Thyroid nodules are very common, affecting about 50-60% of adults.
Like other nodules, thyroid nodules can be benign or cancerous. Benign thyroid nodules account for the majority of cases, about 85-90%. A small proportion of thyroid nodules are malignant, i.e. thyroid cancer.
Why do I have thyroid nodules?
The causes of thyroid nodules are still unclear, but some people are more likely to develop thyroid nodules, and the risk factors include:
- Certain health conditions, such as suffering from autoimmune diseases
- Family history of thyroid nodules
- Insufficient iodine content in the diet
- Living or working in environment with high radiation exposure
What are the symptoms of thyroid nodules?
If the thyroid nodule is small, it usually does not cause any symptoms. In recent years, thyroid nodules are often found incidentally during routine health check-ups or imaging examinations.
However, when the thyroid nodule is relatively large, it may cause the following symptoms:
- A lump being found on the front of the neck
- Foreign body sensation in the anterior neck and throat
- Compressive symptoms caused by thyroid nodules, such as:
- The nodule pressing on the trachea, causing difficulty in breathing
- The nodule pressing on the esophagus, resulting in difficulty in swallowing
- Toxic thyroid nodules producing excess thyroxine and causing hyperthyroidism
- Thyroid cancer with invasion of the recurrent laryngeal nerve that controls the vocal cords, resulting in persistent hoarseness of voice
How to diagnose thyroid nodules?
- Ultrasound of Neck
Ultrasound is an important method to diagnose thyroid nodules. Ultrasound can assess the number, sizes, and locations of thyroid nodules. Most importantly, doctors can assess whether the nodule is benign or malignant based on the following imaging features:- Shape
- Margins
- Composition
- Echogenicity
- Microcalcifications
- Vascularity
- Local invasion
- Blood tests
Blood tests can be done to check whether thyroid hormone levels are normal, including Thyroid Stimulation Hormone (TSH), Free Thyroxine (free T4) and Free Triiodothyronine (free T3), to rule out thyroid function problems.
However, it is important to note that blood tests do not show whether a thyroid nodule is benign or malignant. - Ultrasound-Guided Fine Needle Aspiration Examination
Ultrasound-guided cell aspiration is commonly known as "Fine Needle Aspiration for Cytology" (FNAC). If a thyroid nodule is evaluated as suspicious on ultrasound, FNAC will be needed.
In the process of FNAC, doctor uses ultrasound to guide the needle insertion into the suspicious thyroid nodule while the patient is awake. Then, the doctor will extract cells from the nodule via the needle for pathological analysis.
The cytopathological analysis of thyroid nodules will be evaluated using the Bethesda System for Reporting Thyroid Cytopathology 2017, which divides the cytopathological report of thyroid nodules into 6 grades to assess the risk of malignancy and recommend subsequent treatment.

What is inside a thyroid nodule? Which type of thyroid nodule is more common?
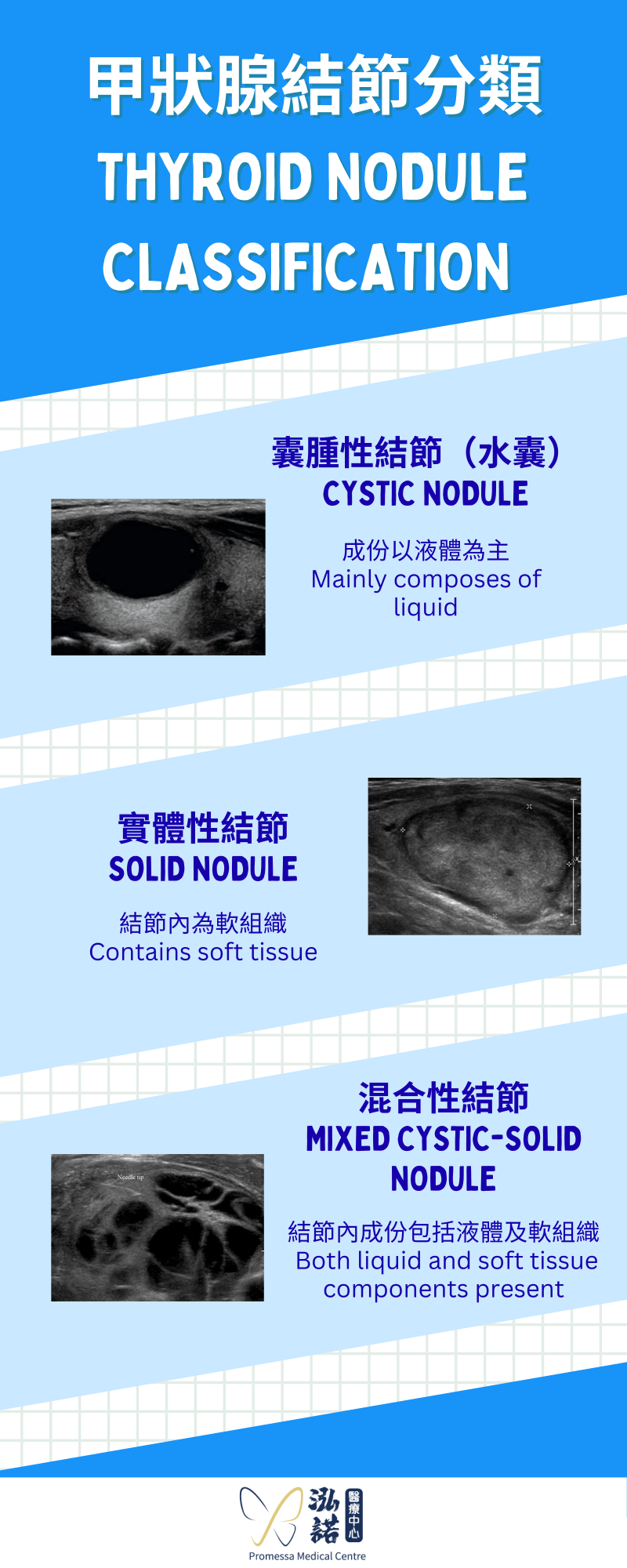
Thyroid nodules can be classified according to the composition of the nodule into:
-
Cystic nodule
Cystic nodule mainly composes of liquid. -
Solid nodule
Solid nodule contains soft tissue within the nodule. -
Mixed cystic-solid nodule
Both liquid and soft tissue components are found in the nodule.
The nature of thyroid nodules cannot be distinguished by appearance or clinical examination alone, it can only be assessed by ultrasound.
Is there a chance that a benign thyroid nodule will become malignant? What are the chances?
If the thyroid nodule is benign, the chance of becoming malignant or thyroid cancer is generally very low, about 1-2%.
Do thyroid nodules have to be surgically treated?
First of all, thyroid nodules cannot be treated with medications, only surgical or interventional treatments are effective in managing the nodules. Before making the decision on the treatment of thyroid nodules, it is important to determine whether the nature of the nodule is benign or malignant.
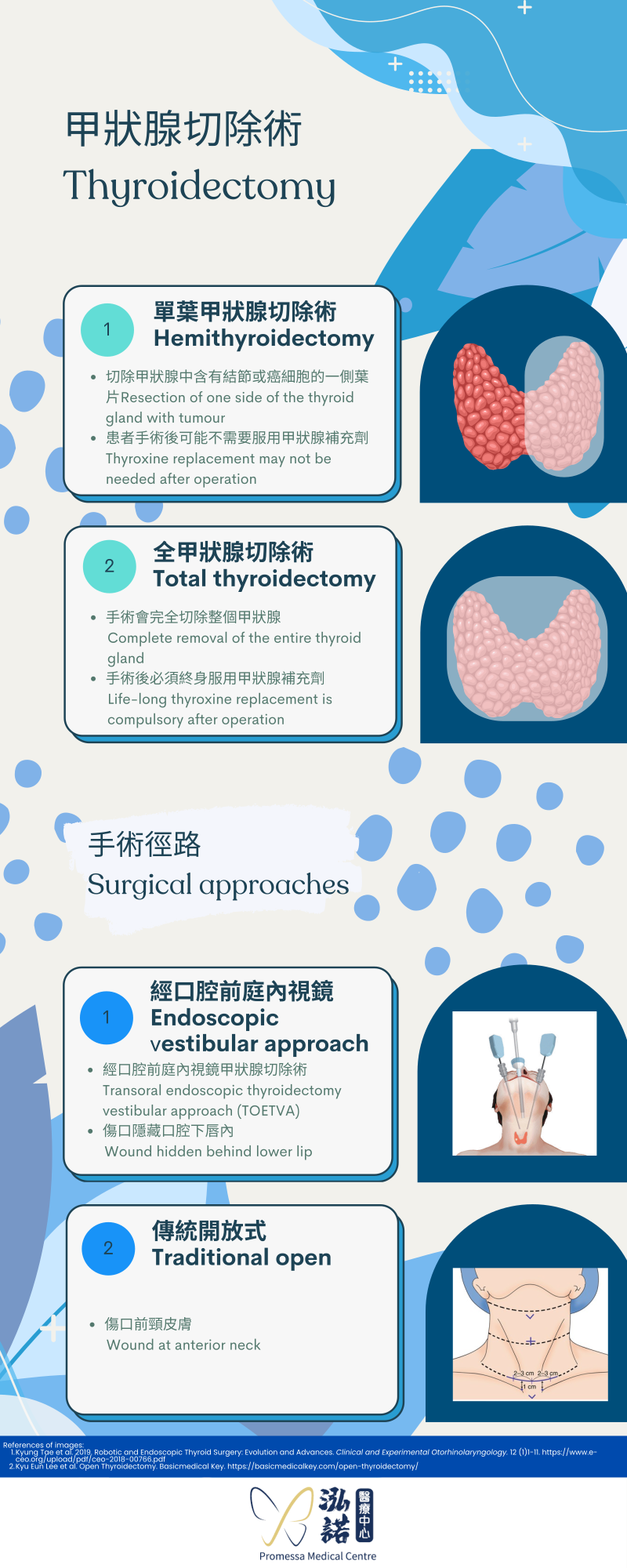
Malignant thyroid nodules, i.e. thyroid cancer, need to be surgically removed.
Benign thyroid nodules, there are more options:
-
Small, thyroid nodules with no compressive symptoms or aesthetic problems
These thyroid nodules can be followed-up with regular ultrasound to monitor the changes in sizes and natures of the nodules. This is because nodules, whether cystic or solid, may deteriorate over time and become larger.
-
Thyroid nodules with compressive symptoms or aesthetic problems
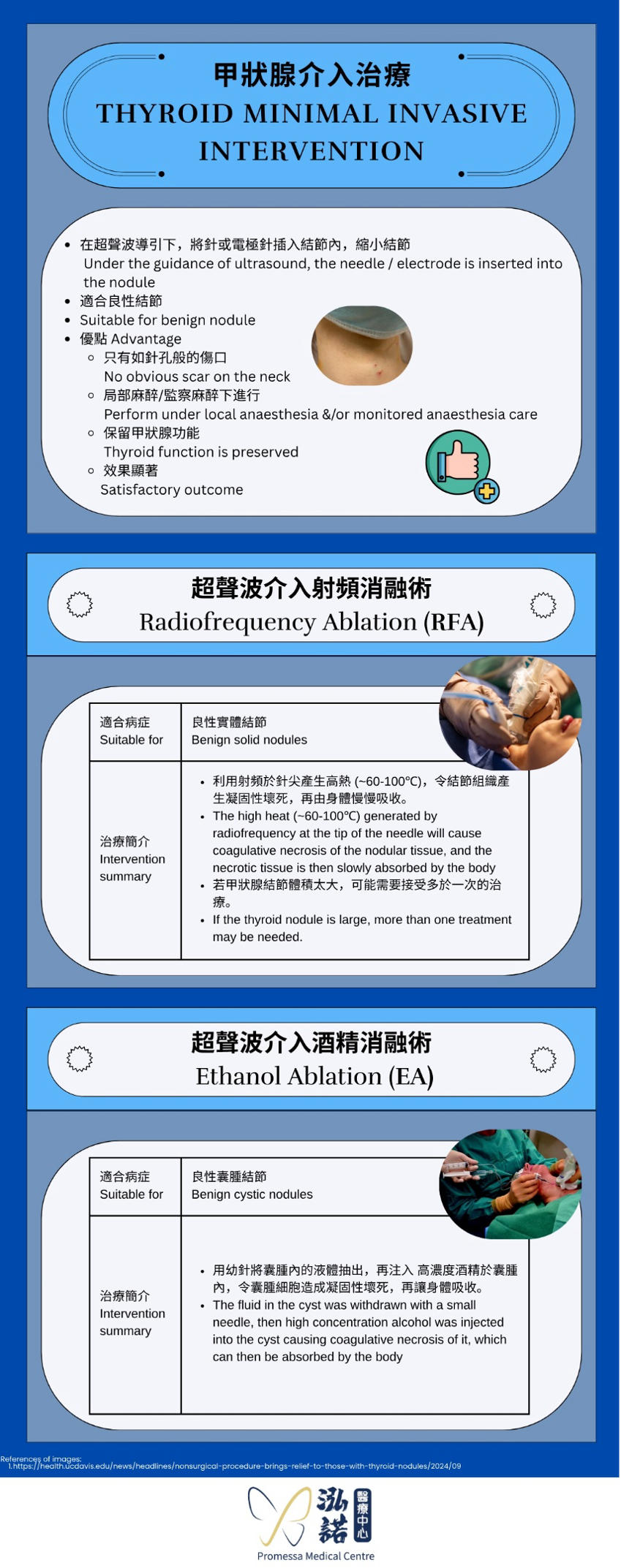
Traditionally, the nodules can be removed by operation via open or endoscopic method (i.e. thyroidectomy). Since the nodule is benign, it is not necessary to have surgery to remove the entire nodule. At present, minimally invasive ultrasound guided interventional treatment can be used to reduce the size of such thyroid nodules, thereby alleviating the symptoms and reducing the chance of recurrence.
The choice of minimally invasive ultrasound guided intervention depends on the nature of the benign thyroid nodule.
What are the minimally invasive treatment options of cystic thyroid nodules?
-
Simple Needle Aspiration
-
Principle:
Direct withdrawal of the fluid from the cyst -
Method:
Draw out the fluid from the cyst with a fine needle to reduce the volume -
Advantages:
- Simple, low surgical risk
- No surgical incision
- Perform under local anesthesia
- No obvious scar on the neck
- Preserve thyroid function
-
Disadvantages:
- Very high recurrence rate (about 80 - 90%)
- May require repeated aspirations
-
Principle:
-
Ethanol Ablation
-
Principle:
Alcohol can cause coagulative necrosis of cyst, which can then be absorbed by the body, thereby shrinking the cyst and reducing the chance of recurrence. -
Procedure:
Under the guidance of ultrasound for positioning, the fluid in the cyst was withdrawn with a small needle to reduce the volume of the nodule, then dehydrated alcohol was injected into the cyst. -
Advantages:
- Short operation time (~15 minutes)
- No surgical incision
- No obvious scar on the neck
- Perform under local anaesthesia
- Low recurrence rate (~5-10%)
- Low surgical risk
- Thyroid function preserved
- Can be discharged from hospital on the same day or next day
-
Who are not suitable for Ethanal Ablation?
- Patients who are allergic to alcohol
- The fluid inside the cyst is too thick to be withdrawn
-
Expected outcome:
If the cyst is not too large, significant volume reduction can be noticed after one course of treatment.
In general, the volume reduction will be seen in about one month to six months after ethanol ablation.
For optimal result, the size of thyroid cyst can be reduced by 85-90% and the chance of recurrence can be as low as 10%. - Any points to note after Ethanol Ablation?
- Avoid strenuous exercise, pressure or massage of the nodule for two weeks after ethanol ablation.
- There are no special or dietary restrictions.
- In the long run, monitor the size of thyroid cyst and watch out for recurrence.
-
Principle:
What are the minimally invasive treatment options of solid thyroid nodules?
Radiofrequency Ablation (RFA)
-
Principle:
Radiofrequency ablation uses the principle of high-frequency vibration to generate high heat (~60-100°C) at the tip of the needle, resulting in coagulative necrosis of the nodule tissue. The necrotic tissue is then slowly absorbed by the body, thereby reducing the volume of the nodule. -
Procedure:
Under the guidance of ultrasound, the RFA electrode is inserted into the solid nodule. The high heat generated by radiofrequency at the tip of the needle will cause coagulative necrosis of the nodular tissue, and the necrotic tissue is then slowly absorbed by the body.
If the thyroid nodule is large, more than one treatment may be needed. -
Advantages:
- No incision, no obvious scar on the neck
- Under local anaesthesia and monitored anaesthesia care, no general anaesthesia required
- Can be discharged from hospital on the same day or next day
- Thyroid function is usually preserved
- Operation time is shorter compared to open excision, usually about 45 to 60 minutes
-
Who are suitable for Radiofrequency Ablation?
- Symptomatic solid nodules that are confirmed to be benign by fine need aspiration for cytology (FNAC).
-
Who are not suitable for Radiofrequency Ablation?
- The nodule was not proven to be benign.
- Mixed nodules: The response of fluid to radiofrequency is not ideal, so if the nodule has more cystic components, the post-ablation effect will be unsatisfactory.
- The nodule is either too large or too low in location. (e.g. extending below the collarbone)
-
Expected outcome:
Radiofrequency ablation can shrink the nodule and reduce recurrence, but it cannot remove the nodule completely. This is because during the operation, in order to protect the nearby normal thyroid tissue and other important organs (such as esophagus, trachea, carotid arteries and jugular veins, nerves, etc.), the electrode needs to be kept at a certain distance from these tissues, so that the tumor will remain and the residual tissue can grow again.
After surgery, the original nodule volume can be reduced by about 30-50% after 3 months and about 70-85% after 6-12 months. - Any points to note during the recovery period of Radiofrequency Ablation?
- Avoid strenuous exercise for two weeks after radiofrequency ablation. Other than that, there are no special or dietary restrictions.
- Avoid vigorous pressure or massage of the nodule.
- In the long run, monitor the size of thyroid nodule and watch out for recurrence.
-
Will the high heat generated by radiofrequency cause pain?
Radiofrequency thyroid ablation is usually performed under monitored anaesthesia care and local anaesthesia, so it is usually painless during the procedure.
What is the treatment of mixed thyroid nodules?
The treatment of mixed thyroid nodules depends on individual circumstances.
Asymptomatic patients can be monitored regularly by ultrasound.
If symptomatic, surgical excision may be considered.
In addition, there are cases where the cyst part is treated with alcohol ablation and the solid part is treated with radiofrequency ablation.